Someday in the future, when Hal passes and if I can get an ok from another guy... I'll light this board up with info. Until then, I'm not posting anything because I made promises not to.
Spidey,
First you demand that I post a description of CTE, so you could explain what is wrong and what is missing, and answer any questions I might have. Now you write: "I'm not posting anything"

That's just not right. I put a lot of time and effort into my recent posts, and I was looking forward to your comments, and the comments from other CTE users out there. I hope some other CTE proponents will come forward if you won't.
Also, from what I know about Hal, he loves sharing information and knowledge, for free!!! Why not help him spread the word about his CTE system while he is still alive ... so more people can benefit. Isn't that a better way to honor him. Isn't that what Hal would want??? Why wait for him to die (that's a terrible thought). I don't understand.
In case you decide to help after all, here's the description you asked me to write:
quoted from dr_dave:
It sounds like we need to start with something. Here is the best I can do at this point, with the limited information available. This is based mostly on the the info posted
here (including the
video from eezbank), and from what I have learned from Hal, Stan, you, and past threads over the years.
DRAFT DESCRIPTION OF THE CTE PROCEDURE
For a “thick hit” (a small cut angle less than 15 degrees) to the left:
- Align the cue 1 tip to the right of the CB center through the right edge of the OB.
- Place the bridge hand down with the cue exactly along this line, using a 10-12 inch bridge length.
- Pivot the cue (without shifting the bridge at all, so the cue rotates about the fixed bridge-pivot point), until the cue is pointed directly through the center of the CB.
- Stroke perfectly straight along this line.
For a “half-ball hit” (close to 30 degrees) to the left:
- Align the cue through the center of the CB and through the right edge of the OB.
- Place the bridge hand down with the cue exactly along this line. The bridge length can be anything for this shot since there is no pivot.
- Stroke perfectly straight along this center-to-edge line.
For a “thin cut” (more than 45 degrees) to the left:
- Align the cue 1 tip to the left of the CB center through the right edge of the OB.
- Place the bridge hand down with the cue exactly along this line, using a 10-12 inch bridge length.
- Pivot the cue (without shifting the bridge at all, so the cue rotates about the fixed bridge-pivot point), until the cue is pointed directly through the center of the CB.
- Stroke perfectly straight along this line.
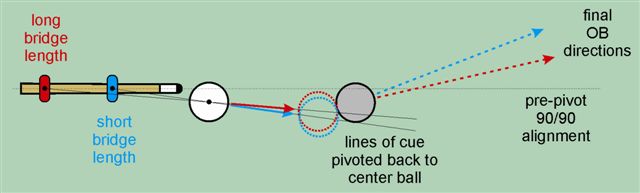
If you follow the procedures above exactly, you will make shots within certain limited ranges of angles. However, you will miss most shots outside of these limited ranges, unless the OB is very close to the pocket and/or the pockets are huge (so significant "pocket cheating" is possible). Now, you can make the procedures work if you compensate a little as the cut angle changes. For example, you can adjust your bridge length (this has a huge effect on the results of the pivot step per Diagram 4 in my
December ‘08 BD article, which is included below), modify the starting tip position a little, pivot slightly less or slightly more relative to the CB center, and/or you can shift your bridge hand slightly during the pivot (e.g., by pivoting with your hips or body) to create a different effective pivot point farther back or closer up from the bridge. You can also “air pivot” where you make subtle changes to all of this stuff intuitively as you come down into the shot (in which case you place your bridge and cue along the required line of aim of the shot with center-ball alignment, without using the separate tip-offset-and-pivot steps). Then, the system can work perfectly for any shot at the table, provided you can judge, perceive, and apply the subtle differences from one shot to another (in which case you don’t need an aiming system).
Hopefully, this is enough of a start to create some useful discussion. I look forward to input from you and others so we can refine this procedure to have it better represent what you think CTE is.
Thank you for your time,
Dave
PS: I put a lot of time into this, so please respond in a constructive way (even if critically constructive), so we can make some progress. In other words, please contribute some of your knowledge and information.
")
